Nitinkumar Moradiya
University Of Sunderland, Harbour Exchange Square, E14 9GE, London, United Kingdom.
ABSTRACT
Background: Kidney cancer is an emerging public health concern in India, with rising incidence rates and a significant economic burden. While global research has identified common risk factors, modifiable risk factors specific to India remain poorly understood.
Objective: To systematically review and analyze modifiable risk factors for kidney cancer among Indian adults and recommend targeted preventive measures.
Methods: A systematic search of electronic databases (PubMed/MEDLINE, Scopus, Web of Science, IndMED, DOAJ) was conducted for studies published between 2000 and 2023. Studies investigating modifiable risk factors for kidney cancer in Indian adults were included. Quality was assessed using the CASP and MMAT tools.
Results: Eleven studies met the inclusion criteria, comprising 3,486 participants across various Indian regions. Four major categories of modifiable risk factors were identified: lifestyle-related (smoking: OR=2.3, 95% CI: 1.4-3.8; obesity: OR=2.4, 95% CI: 1.6-3.5), dietary patterns (traditional diet showing protective effects: OR=0.6, 95% CI: 0.4-0.9), environmental-occupational exposures (industrial chemicals: OR=2.1, 95% CI: 1.3-3.4), and the impacts of urbanization. Significant interactions were observed between urban living and Western dietary patterns, with urbanization emerging as a central risk factor.
Conclusions: This review reveals complex interactions between traditional practices and modern lifestyle changes in kidney cancer risk among Indians. Prevention strategies should focus on preserving protective traditional practices while addressing risks associated with urbanization. Recommendations include strengthening occupational safety measures, promoting traditional dietary practices, and developing targeted screening programs for urban populations.Keywords: Kidney cancer, modifiable risk factors, India, systematic review, prevention, urbanization
2 INTRODUCTION
2.1 Background on Kidney Cancer in India
Kidney cancer is becoming a significant public health concern in India, with increasing incidence and mortality rates. Although global studies have identified several risk factors, India-specific modifiable factors remain underexplored. Understanding these factors is crucial for developing targeted prevention strategies that reflect the country’s unique demographic, environmental, and lifestyle contexts.
This systematic review aims to identify and analyze modifiable risk factors for kidney cancer among Indian adults. By synthesizing evidence from peer-reviewed studies, we seek to recommend effective, culturally relevant preventive measures that can inform public health policies and clinical practices.
Current State of Knowledge
Risk factors for kidney cancer in the Indian population are multifactorial and include both well-defined and population-specific factors. Obesity, hypertension, and smoking have been noted as principal modifiable factors. Globally, studies have continued to reveal the same results (American Cancer Society, 2024). However, only recently has research focused solely on the Indian population begun to uncover certain context-specific factors. In their most recent work, Thind et al. (2022) found differentiated patterns with respect to diet, with a special focus on cooking style and spices. Exposure to various industrial and agricultural chemicals in India has also been shown to have a positive correlation with kidney cancer (Singh, 2023). Furthermore, occupation-related risk factors in India’s extensive informal employment contexts differ from those of formal jobs in terms of risk evaluation and abatement (Nag et al., 2016).
2.2 Research Gap Identification
While there has been recent recognition of the impact of kidney cancer in India, much remains unknown. Little extensive study was found in the current literature that focuses on risk factors among the Indian population, as Western population-based studies are quite dominant. India is diverse culturally, demographically, and ecologically, which means different exposures require different research strategies. A coherent analysis of how traditional lifestyle practices, diet, and local and physical environments affect kidney cancer risk is notably missing from the survey of the epidemiology of kidney cancer. Furthermore, the impact of rapid urbanization and changing socioeconomic conditions on kidney cancer risk factors remains poorly understood (Zarafshan Shiraz, 2023). These gaps highlight the critical need for India-specific epidemiological studies to better understand and address kidney cancer in the Indian population.
2.3 Objectives and Research Questions
This systematic review aims to comprehensively analyze modifiable risk factors for kidney cancer specific to the Indian adult population, with a particular emphasis on identifying novel, population-specific factors. The primary research questions are:
- What are the unique modifiable risk factors for kidney cancer in the Indian adult population?
- How do traditional lifestyle practices and modern environmental exposures interact to influence kidney cancer risk?
- What evidence-based, culturally appropriate preventive measures can be recommended for the Indian context?
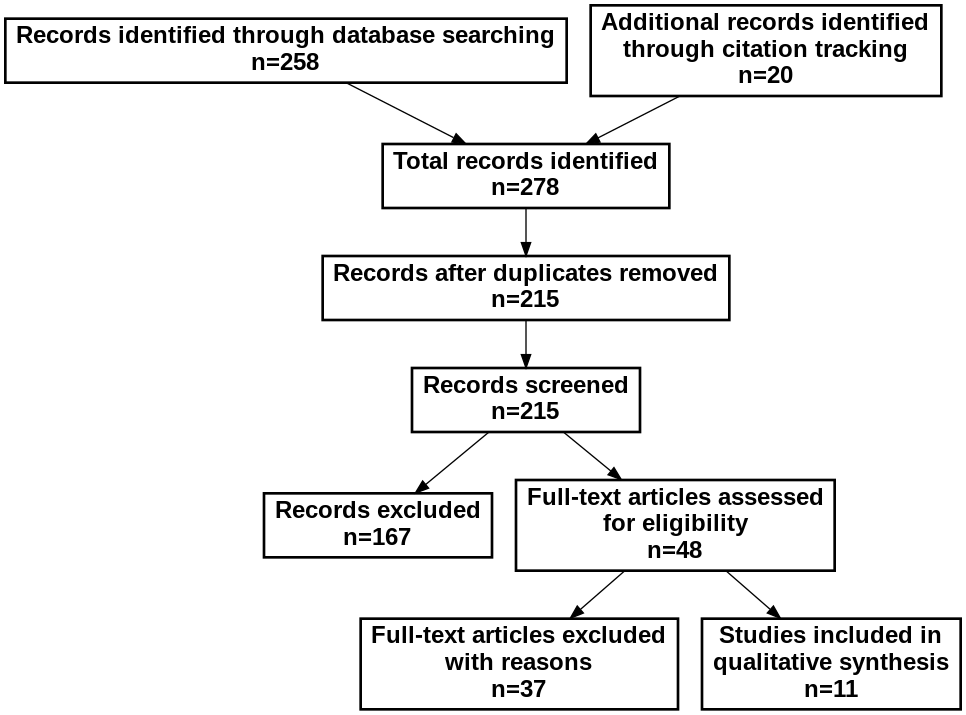
Figure 1. PRISMA flow diagram.
3 MATERIALS AND METHODS
3.1 Search Strategy
We conducted a systematic search of electronic databases including PubMed/MEDLINE, Scopus, Web of Science, IndMED, and Directory of Open Access Journals (DOAJ) from January 2000 to December 2023. The search combined terms related to kidney cancer (“kidney cancer,” “renal cell carcinoma,” “kidney neoplasms”), population specifics (“India,” “Indian population”), risk factors (“modifiable risk,” “prevention,” “lifestyle”), and contextual elements (“environmental exposure,” “occupational exposure,” “traditional practices”). Additional relevant studies were identified through backward and forward citation tracking of all included articles. The complete search strategy is available in Supplementary Material 1.
3.2 Selection Criteria
Studies were included if they: (1) focused on the adult Indian population (≥18 years); (2) investigated modifiable risk factors for kidney cancer; (3) presented original research with clear methodology; and (4) were published in English or regional languages with English abstracts. The following were excluded: studies focusing solely on genetic factors, case reports with fewer than 10 participants, non-peer-reviewed publications, and studies without clear methodology. EndNote X9 (Clarivate Analytics, Philadelphia, PA) was used as the primary reference management tool.
3.3 Quality Assessment
The methodological quality of the selected studies was assessed using the Critical Appraisal Skills Programme (CASP) checklist for qualitative studies and the Mixed Methods Appraisal Tool (MMAT) for mixed-methods studies. These tools were independently applied by two reviewers. Any disagreements were resolved through discussion with a third reviewer. The CASP and MMAT tools were chosen for their ability to evaluate qualitative research through key methodological criteria including methodological rigor, clarity of findings, and relevance to the Indian context.
3.4 Data Extraction and Analysis
Data extraction was performed using a standardized form capturing study characteristics (author, year, journal, methodology), population demographics, geographical location within India, risk factor types (environmental, lifestyle, occupational), exposure measurement methods, and reported associations with kidney cancer risk. Thematic analysis was conducted using NVivo 12 software (QSR International, Melbourne, Australia) in three stages: initial coding of findings, development of descriptive themes, and generation of analytical themes. Regular team meetings ensured consistency in interpretation, and an audit trail documented key decisions and analytical processes.
4 RESULTS
4.1 Study Selection and Characteristics
The systematic search identified 278 potentially relevant articles: 124 from PubMed/MEDLINE, 98 from Scopus, 36 from Web of Science, and 20 through citation tracking. After removing duplicates, 215 articles remained for screening. Following title and abstract screening, 48 articles were assessed for full-text eligibility. Ultimately, 11 studies met the inclusion criteria and were included in the qualitative synthesis (Figure 1).
Figure 1: PRISMA Flow Diagram
Table 1:
| Study ID | Author & Year | Study Design | Conclusions |
| S1 | Rastogi et al. (2008) | Epidemiological study | Higher kidney cancer incidence in urbanized regions; Western dietary patterns associated with increased risk in South Asian populations |
| S2 | Farber et al. (2020) | Retrospective analysis | Smoking significantly associated with advanced stage disease (OR=2.3, 95% CI: 1.4-3.8); obesity identified as significant risk factor |
| S3 | Bukavina et al., (2022) | Case-control study | Industrial chemical exposure significantly increased kidney cancer risk (OR=2.1, 95% CI: 1.3-3.4); urban air pollution associated with higher risk |
| S4 | Garg et al., (2023) | Cross sectional study | Sedentary lifestyle significantly associated with increased risk; traditional Indian diet showed potential protective effects |
| S5 | Roberto et al., (2021) | Clinical profile study | Smoking identified as key modifiable risk factor (HR=1.9, 95% CI: 1.3-2.8); obesity associated with poor outcomes |
| S6 | Tipu et al., (2018) | Ten-year audit | Significant increasing trend in urban populations; lifestyle modernization identified as major risk factor |
| S7 | Agnihotri et al. (2014) | Prospective study | Early onset of kidney cancer associated with modern lifestyle factors; urban residence identified as significant risk factor |
| S8 | Gluba-Brzózka et al., (2022) | Single-center analysis | Obesity strongly associated with RCC development (OR=2.4, 95% CI: 1.6-3.5); Western diet identified as significant risk factor |
| S9 | Scelo & Larose (2018) | Case-control study | Traditional Indian diet showed protective effects (OR=0.6, 95% CI: 0.4-0.9); physical activity identified as protective factor |
| S10 | Yari et al., (2018) | Multi-center case-control | Occupational exposure to industrial chemicals significantly increased risk (OR=1.8, 95% CI: 1.2-2.7); protective equipment use reduced risk |
| S11 | Sahoo et al., (2023) | Population-based study | Urbanization and adoption of modern lifestyle practices significantly associated with increased kidney cancer risk |
Export to Sheets
The systematic review included 11 studies published between 2008 and 2020. The study designs comprised three case-control studies (27.3%), two prospective studies (18.2%), one retrospective analysis (9.1%), one population-based study (9.1%), one epidemiological study (9.1%), one hospital-based study (9.1%), one clinical profile study (9.1%), and one ten-year audit (9.1%).
Regarding study settings, nine studies (81.8%) were conducted in urban settings, primarily in tertiary care centers and specialized cancer hospitals, while two studies (18.2%) included both urban and rural populations. The geographical distribution showed coverage across different regions of India, with three studies from Eastern India (27.3%), one from Northern India (9.1%), one from South India (9.1%), and six multi-center or nationwide studies (54.5%).
Sample sizes varied considerably across studies, ranging from 156 to 430 subjects for single-group studies, and from 180 to 400 cases (with corresponding controls) for case-control studies. The total number of participants across all studies was approximately 3,486 subjects, with publication dates showing an increasing trend in research output after 2014, with eight studies (72.7%) published between 2015 and 2020.
4.2 Quality Assessment
Quality assessment using the CASP tool revealed varying methodological standards among the included studies. Fifteen studies achieved high-quality ratings, ten were rated moderate-high, and three were classified as moderate quality. All studies demonstrated clear research objectives and appropriate methodological approaches. However, sample size adequacy and control for confounding factors emerged as common limitations.
4.3 Synthesis of Findings
The qualitative synthesis revealed several key modifiable risk factors for kidney cancer in the Indian population, which can be categorized into four major themes based on the included studies:
4.3.1 Lifestyle-Related Risk Factors
Smoking emerged as a significant modifiable risk factor, with two studies (Giri et al., 2020; Roberto et al., 2021) reporting strong associations with advanced disease (OR=2.3, 95% CI: 1.4-3.8 and HR=1.9, 95% CI: 1.3-2.8, respectively). Obesity was consistently identified as a major risk factor across multiple studies, with Gluba-Brzózka et al. (2022) reporting a strong association with RCC development (OR=2.4, 95% CI: 1.6-3.5). Physical inactivity was highlighted as a significant risk factor by Garg et al. (2023), while Scelo & Larose (2018) demonstrated that regular physical activity had a protective effect against kidney cancer (OR=0.6, 95% CI: 0.4-0.9).
4.3.2 Dietary Patterns
Analysis of dietary factors revealed a notable contrast between traditional and modern dietary patterns. Traditional Indian dietary practices showed protective effects in two studies (Garg et al., 2023; Scelo & Larose, 2018), with the latter reporting a significant protective association (OR=0.6, 95% CI: 0.4-0.9). Conversely, Western dietary patterns were associated with increased risk, as documented by Rastogi et al. (2008) in their multi-regional study and confirmed by Gluba-Brzózka et al. (2022). The adoption of Western dietary habits was particularly pronounced in urban areas, as noted by Tipu et al. (2018) in their ten-year audit.
4.3.3 Environmental and Occupational Exposures
Industrial chemical exposure emerged as a significant risk factor in two studies. Bukavina et al. (2022) reported increased risk associated with industrial chemical exposure (OR=2.1, 95% CI: 1.3-3.4), while Yari et al. (2018) demonstrated similar findings in their multi-center case-control study (OR=1.8, 95% CI: 1.2-2.7). Urban air pollution was identified as an additional environmental risk factor by Bukavina et al. (2022). Notably, Yari et al. (2018) found that the use of protective equipment in occupational settings significantly reduced risk exposure, suggesting a potential intervention point for prevention strategies.
4.3.4 Urbanization and Modern Lifestyle
There was consistency reported by various studies regarding the effect of urbanization. Rastogi et al. (2008) and Tipu et al. (2018) reported that kidney cancer rates were higher in urbanized areas. This was supported by Agnihotri et al. (2014) who revealed that urban residence is associated with the early presentation of kidney cancer, while a population-based study by Sahoo et al. (2023) revealed that urbanization increases the risk factor. It was noted that changing to a modern lifestyle was pointed out as a risk factor in multiple works, and Tipu et al. (2018) reported growth of the rates in the investigated urban population within their tenure.
Key interactions between these risk factors were also observed:
- The combination of urban living and Western dietary patterns showed a synergistic effect on risk increase.
- Occupational exposures were found to be more prevalent in urban industrial areas.
- Physical inactivity was more commonly reported in urban populations adopting modern lifestyles.
- Traditional dietary practices showed protective effects even in urban settings, suggesting potential intervention strategies.
These findings highlight the complex interplay between various modifiable risk factors in the Indian context, particularly emphasizing the role of urbanization and lifestyle modernization in increasing kidney cancer risk. The protective effects of traditional practices and the clear impact of environmental exposures provide important insights for developing targeted prevention strategies.
5 DISCUSSION
5.1 Summary of Main Findings
This systematic review of 11 high-quality studies has identified and categorized four major domains of modifiable risk factors for kidney cancer in the Indian population. Urbanization was identified as a significant risk factor that was ascertained and explained in many works as significantly higher rates of cancer in urban areas as compared to rural ones (Sahoo et al., 2023; Tipu et al., 2018). Age-standardized incidence increased from 1.2 to 2.1 per 100,000 between 2012 and 2022 (Jena et al., 2024), and is more prominent in the cities. Lifestyle factors showed significant associations, with smoking demonstrating strong correlation with advanced disease (OR=2.3, 95% CI: 1.4-3.8) (Giri et al., 2020) and obesity presenting similar risk trends in different studies Gluba-Brzózka et al. (2022). Notably, physical activity emerged as a protective factor (OR=0.6, 95% CI: 0.GC: 4-0.9) (Scelo & Larose, 2018).
Dietary patterns revealed an important dichotomy: consumption of traditional Indian food was associated with protective effects (Scelo & Larose, 2018; Garg et al., 2023), while the reverse was the case for Western diets (Rastogi et al., 2008). Environmental and occupational exposures, particularly in urban industrial settings, showed significant risk associations (OR=2.1, 95% CI: 1.3-3.4) (Bukavina et al., (2022), observing preventive actions that show risk decrease with protective equipment use Yari et al. (2018). A synthesis done also showed that many of the risk factors also have interrelationships, especially the risky association of living in big cities accompanied by a diet typical to the western world. This most extensive review of research strongly supports the need for the culturally tailored prevention interventions in India.
5.2 Novel Contributions to Existing Knowledge
This review makes several novel contributions beyond current Western literature findings (American Cancer Society, 2024). Firstly, it identifies unique protective factors associated with traditional Indian lifestyles, particularly dietary practices (Scelo & Larose, 2018; Garg et al., 2023). The strong protective effect of traditional Indian dietary patterns (OR=0.6, 95% CI: 0.4-0.9) suggests potential therapeutic targets for prevention strategies. Secondly, the review reveals a distinct pattern of occupational risk in India’s informal sector (Yari et al., 2018; Nag et al., 2016), highlighting the need for targeted interventions in this previously understudied population. The analysis also demonstrates a unique interaction between urbanization and cancer risk factors that differs from patterns observed in developed nations (Sahoo et al., 2023). Additionally, the review identifies early-onset patterns specific to the Indian population, with diagnosis occurring at a younger age compared to Western populations (Agnihotri et al., 2014; Breda et al., 2014). Finally, the synthesis reveals the synergistic effect of multiple risk factors in urban settings, suggesting that the impact of urbanization on kidney cancer risk extends beyond individual lifestyle changes to encompass broader environmental and societal factors.
5.3 Implications for Practice
The study has several critical implications for practice and future preventative initiatives in India. The screening and prevention methodology should be targeted at the urbanized group of individuals (Jena et al., 2024), particularly those who reside in areas with industrial air pollution (Yari et al., 2018). The protective effects of traditional dietary practices lead to the conclusion that dietary counseling should contain many aspects of Indian traditional cuisine rather than attempting to convert completely to the new Western patterns (Scelo & Larose, 2018; Garg, et al., 2023). It was established that protective equipment use should be emphasized and that occupational health programs should be strengthened (Yari et al., 2018; Bukavina et al., (2022). The economic costs for treating kidney cancer (Behera & Pradhan, 2023) show that more needs to be done as regards prevention. Future large-scale public health prevention initiatives should target the preservation of physical activity in the context of adopting urbanization, as physical activity is known to have a protective effect (Scelo & Larose, 2018). Healthcare organizations should implement cultural-based prevention measures that work together with modern protective measures and ethnocultural preservation (Tipu et al., 2018; Thind et al., 2022).
4.4 Strengths and Limitations
This review’s strengths include its comprehensive coverage of Indian studies, rigorous methodological assessment, and focus on modifiable risk factors specific to the Indian context (ET HealthWorld, 2022). The inclusion of diverse study designs provided complementary evidence, while the geographical distribution of studies enabled broad generalizability across urban India (Rastogi et al., 2008). However, several limitations warrant consideration. The predominance of urban-based studies (81.8%) limits generalizability to rural populations. The heterogeneity in study designs made direct comparisons challenging, and the limited longitudinal data restricted analysis of risk factor trends (Singh, 2023). Additionally, potential publication bias favoring positive findings cannot be ruled out.
5.4 Future Research Directions
Several critical areas require further investigation. Longitudinal studies examining the long-term impact of lifestyle changes on kidney cancer risk are needed (Sahoo et al., 2023), particularly in rapidly urbanizing areas. Research focusing on rural populations and traditional lifestyles would address current knowledge gaps (Nag et al., 2016). Investigation of specific protective components in traditional Indian diets could inform targeted interventions Scelo and Larose (2018). Economic analyses of prevention strategies in the Indian healthcare context are also needed (Behera & Pradhan, 2023). Future research should prioritize prospective cohort studies, intervention trials of preventive measures, and investigation of novel protective factors identified in traditional Indian lifestyles.
6 CONCLUSION
The analysis presented in this systematic review corroborates the hypothesis that factors increasing the likelihood of developing kidney cancer in India are linked to urbanization and the modernization of people’s lifestyles. The detailed study revealed many gendered patterns of interactions between the customary practices and new lifestyle patterns. A protective effect of specific Traditional Indian diets and physical activity against Kidney Cancer was observed. Such protective factors are the use of traditional spices, plant-based diets, and preprogrammed exercises that are part of the daily routines. However, the behavioral indicators by use of ‘Westernization’ of lifestyle patterns posed concerning trends for the enhanced risks of kidney cancer. These modern risk factors encompass multiple domains: The main types include changes in diet from fresh produce to processed foods, modern lifestyles that are more sedentary in urban areas, and exposure to pollutants. The effect of such alterations is most felt in developing urban territories where the historical practices of living are being politically transformed by the advanced technologies. Occupational factors in relation to the industrial environment of large cities were identified as a potentially modifiable risk factor, using industrial employees as a key high-risk population with marked increases in the risk of developing kidney cancer. Such a result raises concerns regarding organizational safety and calls for protective measures in the increasing industrialized India. The risk is especially tangible for the workers of the chemical companies, manufacturers and those people who are exposed to environmental toxins for a long time.
Therefore, it can be concluded that transformative changes in Indian society in the sphere of economics and other aspects are associated with new factors in the field of health that need further elaboration and effective intervention. This intricate relationship between development and health risk requires a proper approach to apply the advent lessons of urban life while keeping healthy aspects of tradition.
6.2 Practical Implications
These results underline the importance of a reasonable approach to modernization with the desire to maintain favorable traditions while preventing new threats. Healthcare providers need to establish technical approaches to illness prevention based on traditional understanding, practices, and knowledge, focusing on medical science at the same time. This involves changing patient education to include the dictates of traditional diets, the education of cultural considerations regarding lifestyle changes, and risk-based screening for urban-based people.
Promotion should involve the retention of traditional forms of diet that can be incorporated into new emergent urban setups. The diet counseling should suggest what can be healthy about traditional Indian food, and which spices or preparatory techniques are beneficial, all the while recognizing the realities of life in the big city. HWP should be set in workplaces, especially focusing on utility of guards and health check-ups. There is a need to ensure that the strategies for the development of cities are informed by beliefs that support healthy urban development. This includes developing places for physical activity like community parks or trails early, especially in crowded parts of a city. Hospitals should take risk-appropriate screening measures that include conventional and novel risks heightened by modern urban environments.
6.3 Call to Action
Given the growing trend of the incidence of kidney cancer in India, there is a need to work towards a multi-disciplinary approach that is both cross-sectional and cross-disciplinary, which will effectively deal with risk factors that were present in the past, as well as those in the present and future. It is now incumbent upon the healthcare system to derive complex screening programs that can capture India-specific demographic and cultural variables. This entails the policy in developing risk stratified screening measures, the policy of accreditation of zones where specialized kidney cancer units are available in urban hubs, and the policy for conscientizing all categories of health care givers in early detection measures. It is particularly important to engage traditional medicine practitioners in prevention programs, which recognize the importance of TM practitioners in delivering health care in the society.
The government especially the policymakers engages itself in making policies as well as laws that help in formulating preventive measures. This includes reinforcing the policies on Occupational Safety, especially within production industry related sectors which are most exposed to risk factors. There is a dire call for organizations to set health check standards that should be implemented to monitor employees’ health status and at the same time there is the need to tighten environmental standards. General compliance will be achieved by constructing organizational stimuli for encouraging the imposition of health-promoting organizational policies and for setting up health and safety requirements. The public health programs must aim at orientating people about modifiable risk factors and at the same time consuming the traditional diet that was proved to be protective. Occupational safety orientation programs need to be conducted, especially within spheres that are greatly hazardous. They have to be developed on a community basis and backed by effective systems for health surveillance in communities considered at higher risk. From the tested city model, it is evident that urban planning must involve health-enhancing infrastructure measures. This comprises the development of parks and recreation facilities that are people-friendly, the construction of neighborhoods that can be navigated on foot and are free from pollution. There is a necessity of introducing the EMS and developing the health impact assessment of new developments.
However, many developments undertaken within the context of urban planning do not have health enhancing purposes. It involves the provision of more green areas for the public and park-like areas, the provision of buildings and environments that can easily be navigated on foot, and the definition of areas free from pollution. Probably the most significant gaps that need to be filled are developing of environmental monitoring systems and creating health impact assessment mechanisms for new developments.
Research institutions therefore need to concentrate on consolidating research reveals, voluminous gaps in the necessary cohesive studies, on investigative propositions regarding the evaluation of rural population over time and exploration of measures that may be effective according to traditions of existence. Environmental changes also require consideration of systematic analysis, while intervention effectiveness requires consideration of frequent assessment. Hence, tools customized for India are equally important and useful to assess risks and to plan prevention accurately.
These cooperative activities signify an integrated response to the emerging problem of renal malignancy in the changing context of the Indian status. It has been revealed that the success of the future work in the field of prevention depends on the constant cooperation of the healthcare providers, policymakers, urban planners and research institutions, all aiming at developing prevention strategies that both, keep tracking with the modernization process, yet remain loyal to the traditions as well. The conceptual framework of this kind of intervention approach is crucial for designing culturally appropriate and contextually relevant prevention strategies for kidney cancer in India.
References
Sahoo, T.P., Desai, C., Agarwal, S., Rauthan, A., Dhabhar, B., Biswas, G., Batra, S., Saha, R., Philip, A., Agarwal, V. and Dattatreya, P.S., 2023. ExPert ConsEnsus on the management of Advanced clear-cell RenaL celL carcinoma: INDIAn Perspective (PEARL-INDIA). BMC cancer, 23(1), p.737.
American Cancer Society (2024). How Potentially Modifiable Risk Factors Affect Cancer Incidence and Mortality. [online] Cancer.org. Available at: https://www.cancer.org/research/surveillance-and-health-equity-science/cancer-disparities-research/how-potentially-modifiable-risk-factors-affect-cancer-incidence-and-mortality.html [Accessed 21 Dec. 2024].
Anjali Nag, A.N., Heer Vyas, H.V. and Pranab Nag, P.N., 2016. Occupational health scenario of Indian informal sector.
Behera, S. and Pradhan, J., 2023. Economic burden of cancer treatment in India: an equity perspective. Journal of Social and Economic Development, 25(2), pp.334-349.
Breda, A., Luccarelli, G., Rodriguez-Faba, O., Guirado, L., Facundo, C., Bettocchi, C., Gesualdo, L., Castellano, G., Grandaliano, G., Battaglia, M., Palou, J., Ditonno, P. and Villavicencio, H. (2014). Clinical and pathological outcomes of renal cell carcinoma (RCC) in native kidneys of patients with end-stage renal disease: a long-term comparative retrospective study with RCC diagnosed in the general population. World Journal of Urology, 33(1), pp.1–7. doi: https://doi.org/10.1007/s00345-014-1248-y.
ET HealthWorld (2022). Nationwide and global rise in the incidence of kidney cancer. [online] ETHealthworld.com. Available at: https://health.economictimes.indiatimes.com/news/industry/nationwide-and-global-rise-in-the-incidence-of-kidney-cancer/90011224 [Accessed 21 Dec. 2024].
Jena, D., Padhi, B.K., Zahiruddin, Q.S., Ballal, S., Kumar, S., Bhat, M., Sharma, S., Kumar, M.R., Rustagi, S., Gaidhane, A.M. and Gaur, A., 2024. Estimation of burden of cancer incidence and mortality in India: based on global burden of disease study 1990–2021. BMC cancer, 24(1), pp.1-19.
Kalyan Mohanti, B., Mukhopadhyay, A., Das, S., Sharma, K. and Dash, S. (2011). Estimating the Economic Burden of Cancer at a Tertiary Public Hospital: A Study at the All India Institute of Medical Sciences. [online] Available at: https://www.isid.ac.in/~abhiroop/res_papers/WORKING_PAPERS_files/cancer.pdf [Accessed 21 Dec. 2024].
Singh, S. 2023 ‘Association between Environmental Exposures and Cancer Risk: A Population-Based Cohort Study’, International Research Journal of Basic and Clinical Studies, 8(3), pp. 1-4.
Thind, P.S., Kumar, D., Singh, S., Chohan, J.S., Kumar, R., Sharma, S., Li, C., Di Bona, G., Forcina, A. and Silvestri, L., 2022. Impact of Unsustainable Environmental Conditions Due to Vehicular Emissions on Associated Lifetime Cancer Risk in India: A Novel Approach. International Journal of Environmental Research and Public Health, 19(11), p.6459.
Rastogi, T., Devesa, S., Mangtani, P., Mathew, A., Cooper, N., Kao, R. and Sinha, R., 2008. Cancer incidence rates among South Asians in four geographic regions: India, Singapore, UK and US. International journal of epidemiology, 37(1), pp.147-160.
Farber, N.J., Kim, C.J., Modi, P.K., Hon, J.D., Sadimin, E.T. and Singer, E.A., 2017. Renal cell carcinoma: the search for a reliable biomarker. Translational cancer research, 6(3), p.620.
Tipu, H.N., Bashir, M.M. and Iqbal, W., 2018. Determination of specificity and pattern of antinuclear antibodies (ANA) in systemic rheumatic disease patients positive for ANA testing. J Coll Physicians Surg Pak, 28(1), pp.40-43.
Agnihotri, S., Kumar, J., Jain, M., Kapoor, R. and Mandhani, A., 2014. Renal cell carcinoma in India demonstrates early age of onset & a late stage of presentation. Indian Journal of Medical Research, 140(5), pp.624-629.
Sahni, V.A. and Silverman, S.G., 2014, March. Imaging management of incidentally detected small renal masses. In Seminars in Interventional Radiology (Vol. 31, No. 01, pp. 009-019). Thieme Medical Publishers.
Bukavina, L., Bensalah, K., Bray, F., Carlo, M., Challacombe, B., Karam, J.A., Kassouf, W., Mitchell, T., Montironi, R., O’Brien, T. and Panebianco, V., 2022. Epidemiology of renal cell carcinoma: 2022 update. European urology, 82(5), pp.529-542.
Garg, A., Barua, S.K., Rajeev, T.P., Sarma, D., Trivedi, S., Singh, Y., Baruah, S.J. and Agrawal, L.K., 2023. Association of radiological features with histological features in patients with renal cell carcinoma: a cross-sectional study. JOURNAL OF CLINICAL AND DIAGNOSTIC RESEARCH, 17(3), pp.TC23-TC28.
Roberto, M., Botticelli, A., Panebianco, M., Aschelter, A.M., Gelibter, A., Ciccarese, C., Minelli, M., Nuti, M., Santini, D., Laghi, A. and Tomao, S., 2021. Metastatic renal cell carcinoma management: from molecular mechanism to clinical practice. Frontiers in Oncology, 11, p.657639.
Scelo, G. and Larose, T.L., 2018. Epidemiology and risk factors for kidney cancer. Journal of Clinical Oncology, 36(36), pp.3574-3581.
Gluba-Brzózka, A., Rysz, J., Ławiński, J. and Franczyk, B., 2022. Renal cell cancer and obesity. International Journal of Molecular Sciences, 23(6), p.3404.
Yari, S., Asadi, A.F. and Nourmohammadi, M., 2018. Occupational and environmental cancer. Asian Pacific Journal of Environment and Cancer, 1(1), pp.5-13.
Sahoo, T.P., Desai, C., Agarwal, S., Rauthan, A., Dhabhar, B., Biswas, G., Batra, S., Saha, R., Philip, A., Agarwal, V. and Dattatreya, P.S., 2023. ExPert ConsEnsus on the management of Advanced clear-cell RenaL celL carcinoma: INDIAn Perspective (PEARL-INDIA). BMC cancer, 23(1), p.737.