
May 29–June 2, 2026 | Chicago, IL
Senthil Pazhanisamy, BPharma, MS, PhD.
Overview
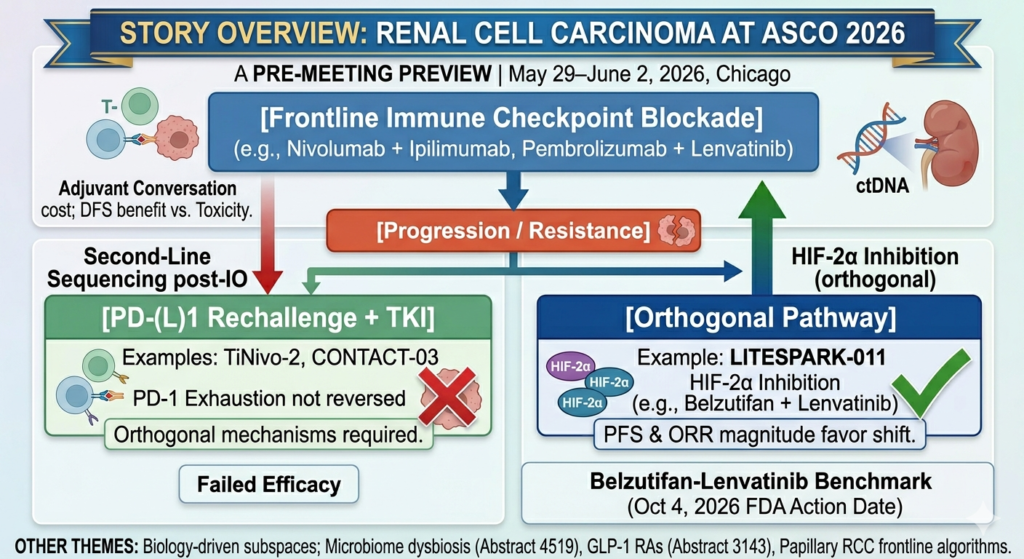
The 2026 ASCO Annual Meeting arrives at a critical inflection point for renal cell carcinoma (RCC). The February ASCO GU Symposium in San Francisco delivered a rapid sequence of headline readouts—LITESPARK-022 in the adjuvant setting, LITESPARK-011 after immune checkpoint blockade (ICB), the disappointing LITESPARK-012 in first-line disease, and longer follow-up of CheckMate 214. Collectively, these data reshaped our understanding of hypoxia-inducible factor-2α (HIF-2α) inhibition, sequencing post-PD-(L)1 exposure, and the long-term durability of frontline doublet standards. While the Chicago meeting may not deliver another single explosive bombshell on the scale of LITESPARK-022, it will critically sharpen, complicate, and challenge those winter conclusions.
Three core themes deserve particular attention from the kidney cancer community:
- A Crowded Adjuvant Conversation: The post-nephrectomy space is no longer a one-trial monologue. The RAMPART trial’s durvalumab monotherapy arm reads out for the first time, while a highly anticipated ctDNA-based reanalysis of KEYNOTE-564 directly confronts the reality of overtreatment in intermediate-risk disease.
- Contesting the Second-Line: The post-immunotherapy second-line space—where belzutifan plus lenvatinib has established a formidable contemporary benchmark—gains long-term confirmatory data from the final analysis of TiNivo-2.
- The Rise of Practical Biology: The gut microbiome enters mainstream RCC discourse as a predictive rather than purely modulatory asset via the City of Hope CBM588 dysbiosis analysis.
Adjuvant Therapy: De-escalation and Tiered Intensity
Adjuvant pembrolizumab, established by KEYNOTE-564, has anchored post-nephrectomy decision-making for nearly five years as the only systemic therapy demonstrating both disease-free survival (DFS) and overall survival (OS) benefits. ASCO GU 2026 provided its first true combination competitor via LITESPARK-022, revealing that adding belzutifan to pembrolizumab improved DFS over immunotherapy alone ($\text{HR } 0.72$; $95\%\text{ CI}$, $0.59\text{–}0.87$; $P = .0003$). The Annual Meeting will now dictate how these strategies are operationalized in clinical practice.
RAMPART Arm B: Isolating the Cost of CTLA-4 Blockade
The UK-led RAMPART platform trial (NCT03288532) previously demonstrated at ESMO 2025 that adjuvant durvalumab plus tremelimumab significantly improved 3-year DFS over active monitoring ($\text{HR } 0.65$; $95\%\text{ CI}$, $0.45\text{–}0.93$; $P < .01$). However, a steep toxicity cost—Grade $\ge 3$ adverse events hitting $40\%$ versus just $8\%$ in the control arm—has heavily tempered clinical enthusiasm.
At ASCO 2026, the presentation of RAMPART Arm B (durvalumab monotherapy vs. active monitoring) will provide two vital clinical insights:
- It tests whether single-agent PD-L1 blockade can safely join pembrolizumab in the adjuvant toolset, offering an alternative for patients with access or tolerability restrictions to the approved Merck regimen.
- By triangulating this data with the existing doublet arm, it cleanly isolates the incremental therapeutic contribution of tremelimumab—and weighs it against the toxicity price extracted by dual checkpoint inhibition.
The Clinical Takeaway: A positive monotherapy result with a benign safety profile positions RAMPART as a flexible, tiered platform. A negative result conversely places the entirety of the platform’s efficacy on tremelimumab’s shoulders, forcing a difficult calculation regarding toxicity-adjusted value.
KEYNOTE-564 ctDNA Reanalysis: Confronting Overtreatment
Perhaps no abstract in this year’s adjuvant lineup will provoke more immediate practical reflection than the ctDNA-stratified reanalysis of KEYNOTE-564. Historically, KEYNOTE-564 enrolled patients strictly by clinicopathologic risk markers (pT3, pT4, N+, or M1 NED) without molecular minimal residual disease (MRD) stratification. Consequently, many patients who would never have recurred are likely receiving unnecessary systemic therapy.
If post-nephrectomy ctDNA status successfully isolates a subgroup whose pembrolizumab benefit is entirely concentrated—or utterly absent—treatment paradigms could shift immediately. Conversely, identifying ctDNA-positive patients who are destined to recur early provides clinicians with the exact cohort justified for aggressive adjuvant intensification (such as the LITESPARK-022 doublet). The era of choosing adjuvant therapy based purely on tumor size and lymph node status is rapidly closing.
Post-Immunotherapy Second Line: Orthogonal Mechanisms
The second-line space post-frontline ICB has historically defaulted to historical VEGFR-TKI monotherapies (cabozantinib, axitinib, or tivozanib). LITESPARK-011 disrupted this default at ASCO GU 2026 by proving that belzutifan plus lenvatinib significantly extended median PFS over cabozantinib monotherapy ($14.8$ vs. $10.7$ months; $\text{HR } 0.70$; $95\%\text{ CI}$, $0.59\text{–}0.84$) in the post-PD-(L)1 setting, setting up an FDA action date of October 4, 2026.
TiNivo-2 Final Analysis (Abstract 4555): Closing the Door on Rechallenge
Dr. Robert Motzer (MSK) will present the final analysis of the Phase 3 TiNivo-2 trial evaluating tivozanib plus nivolumab versus tivozanib alone after IO progression. The primary readout verified that checkpoint rechallenge adds no clinical value over TKI monotherapy, aligning with the negative results of CONTACT-03.
The maturation of this data solidifies an essential biological truth: the immunologic exhaustion generated during frontline PD-(L)1 therapy cannot be bypassed simply by switching to an alternate anti-PD-1 agent. Next-line regimens must leverage genuinely orthogonal mechanisms of action—like HIF-2α inhibition—rather than duplicating prior targets.
Where Tivozanib Sits Now
The long-term outcomes from TiNivo-2 will clarify tivozanib’s modern sequencing niche. Approved for relapsed/refractory advanced RCC after two or more prior lines, tivozanib presents a highly favorable, predictable safety profile relative to cabozantinib—notably causing less hand-foot syndrome and severe diarrhea. It remains a foundational tool for frail, older, or heavily pre-treated patients, even as combination doublets move into the immediate second-line slot.
Biology-Driven Subspaces & Cross-Cutting Signals
CBM588 and the Microbiome (Abstract 4519)
The City of Hope group will report on baseline microbial dysbiosis as a definitive predictor of benefit from CBM588 (a live bacterial product, Clostridium butyricum) alongside frontline ICB doublets. While previous small, randomized trials from Sumanta Pal’s program demonstrated that CBM588 enhances T-cell priming and extends PFS, Abstract 4519 transitions the conversation from safety to precision selection: can we identify exactly which patients’ gut microbiomes require therapeutic modulation? CBM588 remains an investigational agent, but the trial marks a crucial step toward deployable microbiome biomarker companion tools.
Frontline Strategies in Papillary RCC (Education Session)
Non-clear cell histologies remain a persistent gap in systemic evidence bases. Papillary RCC, the most common non-clear cell variant, has historically been treated via clinical extrapolation from clear cell protocols. A dedicated education session led by Charles Nguyen (City of Hope) will synthesize the field’s shift toward MET-pathway targeting and cabozantinib-based combinations (refined by the SWOG 1500/PAPMET2 programs), carving out a separate, histology-specific frontline algorithm.
The GLP-1 Receptor Agonist Signal (Abstract 3143)
A massive real-world analysis of over 10,000 cancer patients tracking GLP-1 receptor agonist (GLP-1 RA) use has uncovered a striking retrospective association with improved overall survival across several metabolic-heavy malignancies, including RCC. While retrospective pharmacoepidemiology is consistently vulnerable to confounding factors (such as baseline metabolic phenotypes, weight changes, and indication biases), kidney cancer clinicians must track this signal closely. A significant percentage of advanced RCC patients suffer from baseline metabolic syndrome, and understanding how GLP-1 RAs intersect with the vascular and metabolic toxicities of frontline IO-TKI doublets will be a common point of discussion in the clinic.
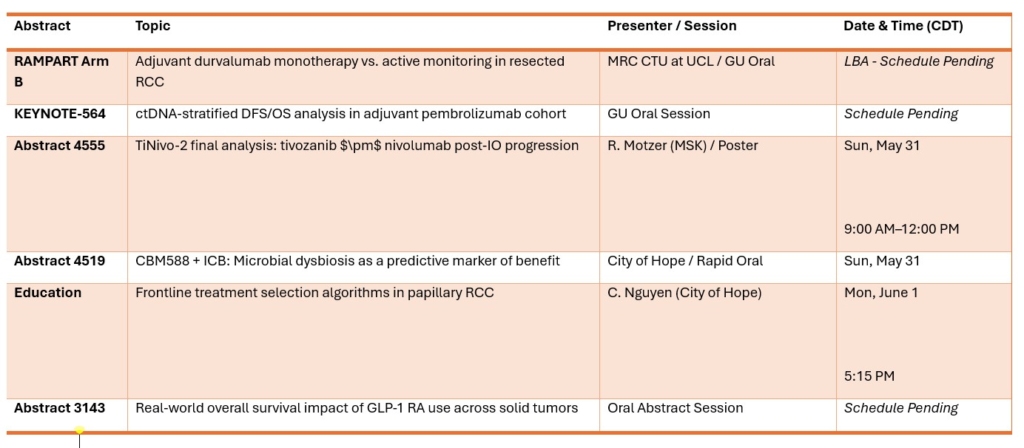
Abstracts at a Glance